Here’s a coverage policy for Galafold (migalastat), a treatment for Fabry disease, from BCBS Illinois:
Policy reference
- Plan: BCBS Illinois
- PBM: Prime Therapeutics
- Line of business: Commercial
- Drug: Galafold (migalastat)
- Effective date: July 1, 2025
- Accessed: January 5, 2026
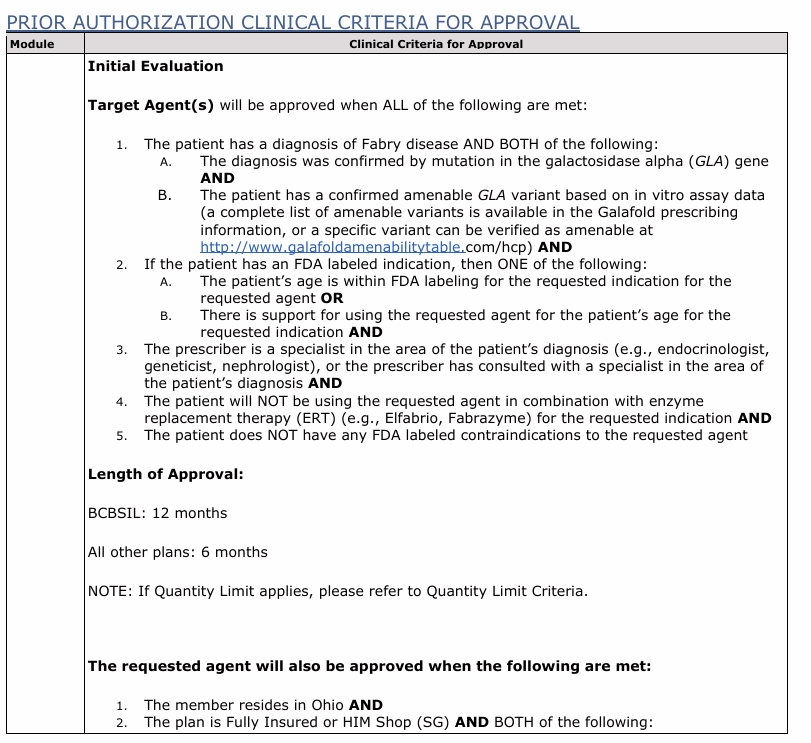
It’s actually a well-structured policy. Look at what they made explicit:
- Diagnosis confirmed by GLA mutation ✓
- Amenable variant verified via linked table ✓
- Specialist prescriber required ✓
- No concurrent enzyme replacement therapy ✓
But then there’s criterion 2A:
“The patient’s age is within FDA labeling for the requested indication for the requested agent.”
Why is this out-referenced?
The asymmetry
The variant amenability table—which actually changes as assay data accumulates—gets a direct URL. You can click it and verify.
Age—which is stable for the life of the drug—gets deferred to “FDA labeling” as an interpretive exercise.
That’s backwards.
Age is not ambiguous data. It is stable, binary, and easily specified.
What does “FDA labeling” even say?
We checked. Here’s what you find:
- Indication statement: “adults with Fabry disease” — implies 18+
- Pivotal trial population: patients aged 16–68 were enrolled
- Dosage section: no age-specific guidance
- Geriatric use: limited data in patients over 65
So which number governs?
The policy doesn’t say.
The label doesn’t say cleanly either.
A 17-year-old with confirmed Fabry disease and an amenable variant could be denied because “adult = 18+.”
A 75-year-old could be approved despite being outside the studied population entirely.
The out-reference doesn’t resolve this. It creates it.
This isn’t an accusation
I’m not claiming this is fraud, abuse, or intentional. It’s likely a template convention inherited from Prime Therapeutics that propagates across dozens of policies without anyone questioning whether it fits each drug.
But conventions have consequences.
Every out-reference is an interpretive layer.
Every interpretive layer is a potential denial or approval.
Every wrong denial is a burden on the clinician, the patient, and the pharmacy—to figure out what the policy actually requires.
What “collapsed” looks like
Here’s criterion 2A with the indirection removed:
“The patient’s age is within FDA labeling for the requested indication for the requested agent.”
→ “Patient is 18 years of age or older.”
Or, if the committee wants to honor the evidence base:
“Patient is 16–68 years of age, consistent with the studied population.”
Either position is defensible.
What’s harder to defend is relying on “FDA labeling” to answer a question it doesn’t clearly resolve.
Why this matters
This is one policy, one drug, one set of clauses that introduce ambiguity. But the pattern is everywhere.
Out-referencing stable information while specifying dynamic information is a design choice that adds friction without adding clarity. It shifts interpretive burden downstream—to people with less time, less access, and less power to contest.
I’m not here to name villains.
I’m here to collapse the indirection.
That’s what Policy Vault is for.
The test this post has to pass
- Does it reduce information asymmetry?
Yes—you now know what the label actually says. - Does it increase contestability?
Yes—you can cite the trial population in an appeal. - Is it falsifiable?
Yes—check the label yourself. - Does it offer navigation, not just exposure?
Yes—”here’s what the collapsed criterion looks like.” - Does it avoid collateral damage?
Yes—no individuals named, just a system pattern.
If the work passes that test, it’s earned.